Testosterone is a male sex hormone that is involved in the development of the genitals and the appearance of secondary sex characteristics in men.
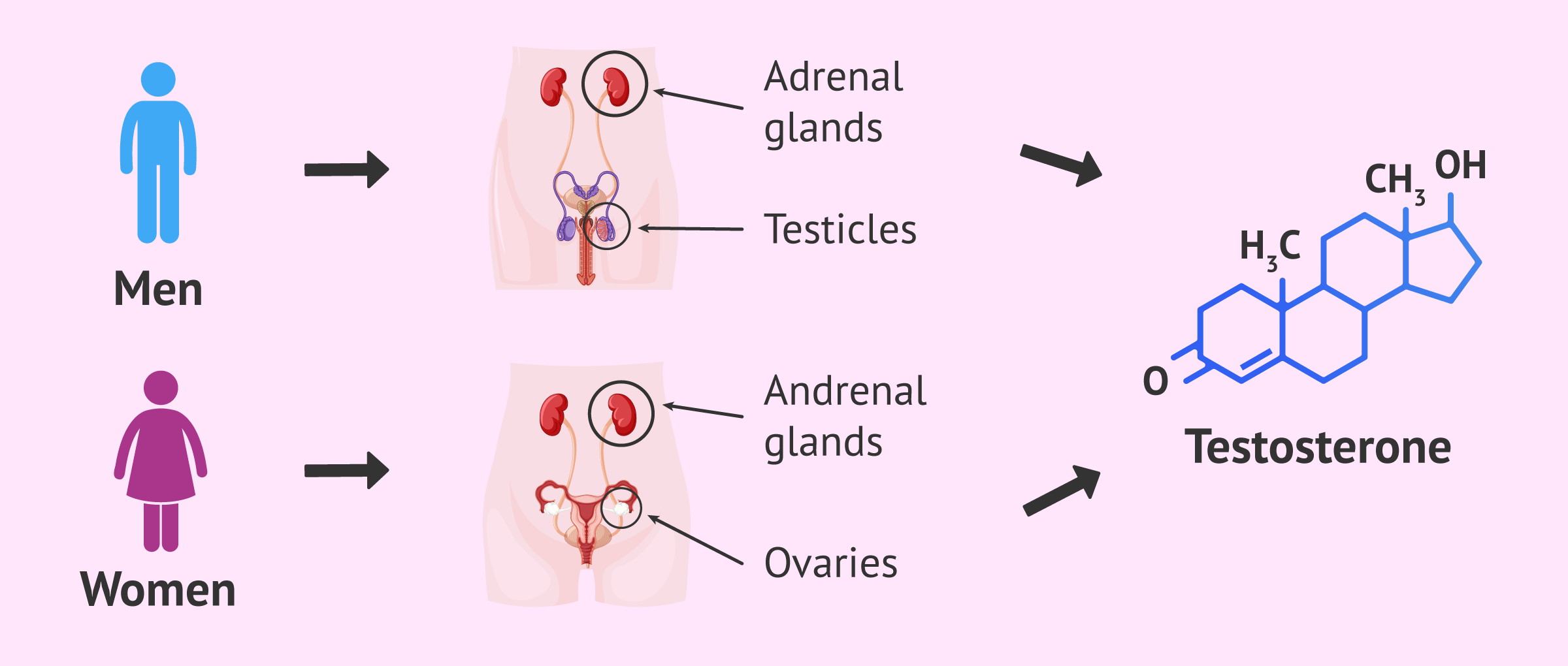
It is an anabolic steroid that is produced mainly by the testicles, although a small amount is also released by the adrenal glands.
Testosterone is the androgenic hormone par excellence, but doesn’t exclusively occur in men. Women's ovaries and adrenal glands also produce a lesser amount of testosterone and are related to increased libido.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 4.
- 4.1.
- 4.2.
- 5.
- 5.1.
- 5.2.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 7.
- 8.
- 9.
- 10.
What is testosterone?
Testosterone is a steroid hormone because it comes from cholesterol. Specifically, testosterone is part of the group of hormones called androgens and is the main male sex hormone.
Other hormones in the androgen group are dehydroepiandrosterone sufato (DHEAS), dehydroepiandrosterone (DHEA), androstendione and dihydrotestosterone (DHT). However, DHEAS, DHEA and androstenedione are really hormone precursors, as they need to be converted to testosterone and DHT in order to express their effects.
Another type of steroid sex hormones are estrogens. Traditionally estrogens are known as female hormones and androgens are known as male hormones, but both types are present in both women and men.
Where and how is testosterone produced?
In men, about 95% of testosterone is produced by the Leydig cells of the testicles.
This process is known as steroidogenesis and is perfectly regulated by the hypothalamus and the pituitary gland of the brain through the hormone LH.
Once expelled into the blood, testosterone travels through the bloodstream bound to other proteins: sex hormone binding globulin (SHBG) and albumin. Because of this binding, the function of testosterone is inhibited because it cannot bind to its receptor.
On the other hand, a small amount of testosterone remains free in the blood and is active to carry out its function.
Bioavailable testosterone is the sum of free testosterone and testosterone bound to albumin, as this protein has a low binding affinity to testosterone and can therefore release it quickly.
In the case of women, testosterone is produced by the teak cells of the ovaries and by the adrenal glands.
Function of testosterone
Testosterone appears in the first weeks of embryonic development and is responsible for the virilization of the male fetus.
This hormone plays a very important role in the development of the male reproductive system and in the development of his secondary sexual characteristics.
On the other hand, testosterone also intervenes in the sexuality of men and women, is very important for bone health, has anti-inflammatory and antioxidant action and also has favorable effects on blood vessels.
In the following sections we will discuss in greater detail which are the functions of testosterone for both sexes.
In men
In addition to the fetal period, testosterone becomes especially important in men after puberty. From the age of 11-13, testosterone production begins to increase in children and is maintained for the rest of their lives.
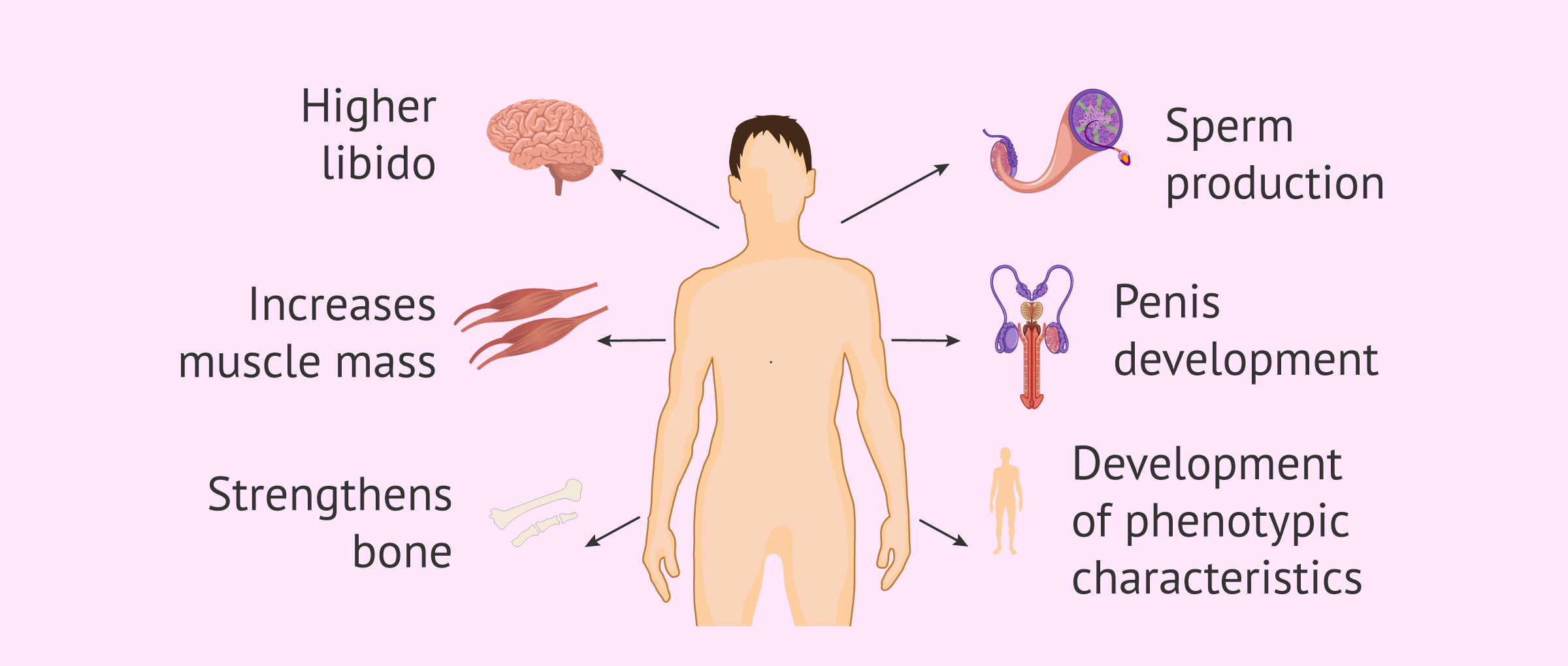
Below, we will detail the functions of testosterone in men's bodies:
- Promotes the development and growth of the penis, testicles, scrotum, and sexual secretory glands.
- Promotes the appearance of phenotypic characteristics of men: beard and hair on the body, deeper voice, growth of Adam's apple, etc..
- Stimulates the sperm production (spermatogenesis) in the seminiferous tubules and thus developing male fertility.
- It stimulates the maturation of spermatids to become spermatozoa and the definitive formation of semen.
- Develops bone growth and prevents osteoporosis.
- Promotes increased muscle mass and strength.
- Increases libido or sexual desire.
In women
In the case of women, they also produce testosterone and other androgens that are important for maintaining ovarian function, bone metabolism, cognitive function, and sexual function.
As far as female reproduction is concerned, the role of androgens is not entirely clear, although it is necessary to maintain adequate levels for correct ovarian functioning.
Androgens play a fundamental role in follicular development, so high levels can lead to excessive growth with dysfunctional formation of antral follicles, as in polycystic ovary syndrome (PCOS). On the other hand, too low levels of androgens are associated with low ovarian response and ovarian insufficiency.

Apart from this, androgens have been shown to increase levels of receptors for the FSH hormone in the follicles, which is responsible for inducing follicular growth.
Testosterone values
Hormone analysis is one of the basic diagnostic tests for the study of fertility in both men and women.
One of the hormones that is quantified is testosterone, as it can provide information on causes of infertility, decreased sexual desire, irregular menstrual cycles, testicular tumors, etc..
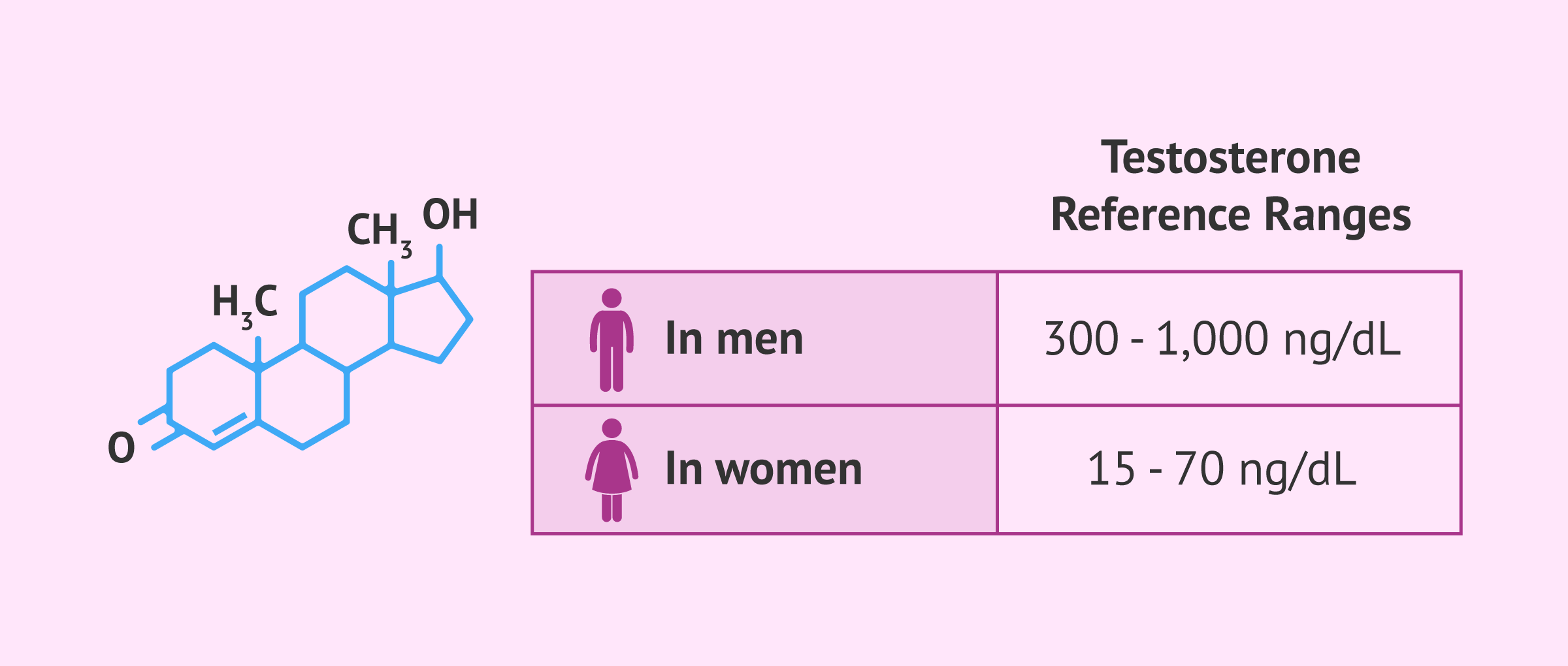
An adult man produces about 20 times more testosterone than an adult female. Specifically, these are the testosterone values that are considered normal:
- In men
- between 300-1,000 ng/dL.
- In woman
- between 15-70 ng/dL.
Furthermore, having a reading within this ‘normal’ range does not automatically rule out an imbalance. For this reason, a specialist will never assess these figures in isolation; they will always consider them alongside clinical symptoms and the rest of the hormonal profile in order to provide an accurate and personalised diagnosis.
Low testosterone levels
Testosterone deficiency in men has several consequences on different physiological processes such as those listed below:
- Difficulty in maintaining an erection
- Lack of libido
- Low sperm count (oligozoospermia)
- Decreased strength and loss of muscle mass
- Fat accumulation and breast enlargement
- Decreased bone mineral density and osteoporosis
- Energy loss and increased fatigue

Men presenting those symptoms are recommended to make an appointment at a specialist in order to undergo hormonal exams and have their case evaluated.
If after several tests the doctor finds that the testosterone levels are low and the clinical manifestations cannot be contributed to any other cause, hormone therapy with testosterone may be applied.
High testosterone levels in men
There is often a false belief that "the more testosterone, the more virility and fertility". However, an excess of this hormone in men can, in fact, be one of the greatest enemies when trying to achieve a pregnancy.
Having naturally high testosterone levels well above normal limits is rare and, when it occurs, it is usually due to alterations in the adrenal glands or, in rare cases, testicular tumors.
However, the most common cause of excessively high blood testosterone levels is of external origin. The consumption of anabolic steroids (very common in the bodybuilding and fitness environment) or the use of Testosterone Replacement Therapies (TRT) without adequate medical supervision can cause an imbalance in testosterone levels in men.
How to increase testosterone?
When a blood test confirms that testosterone levels are below the optimal range, or if you are simply looking to improve hormonal health to support fertility, it is completely normal to wonder what the next step should be.
Broadly speaking, there are two main paths discussed below.
Tips to improve testosterone levels
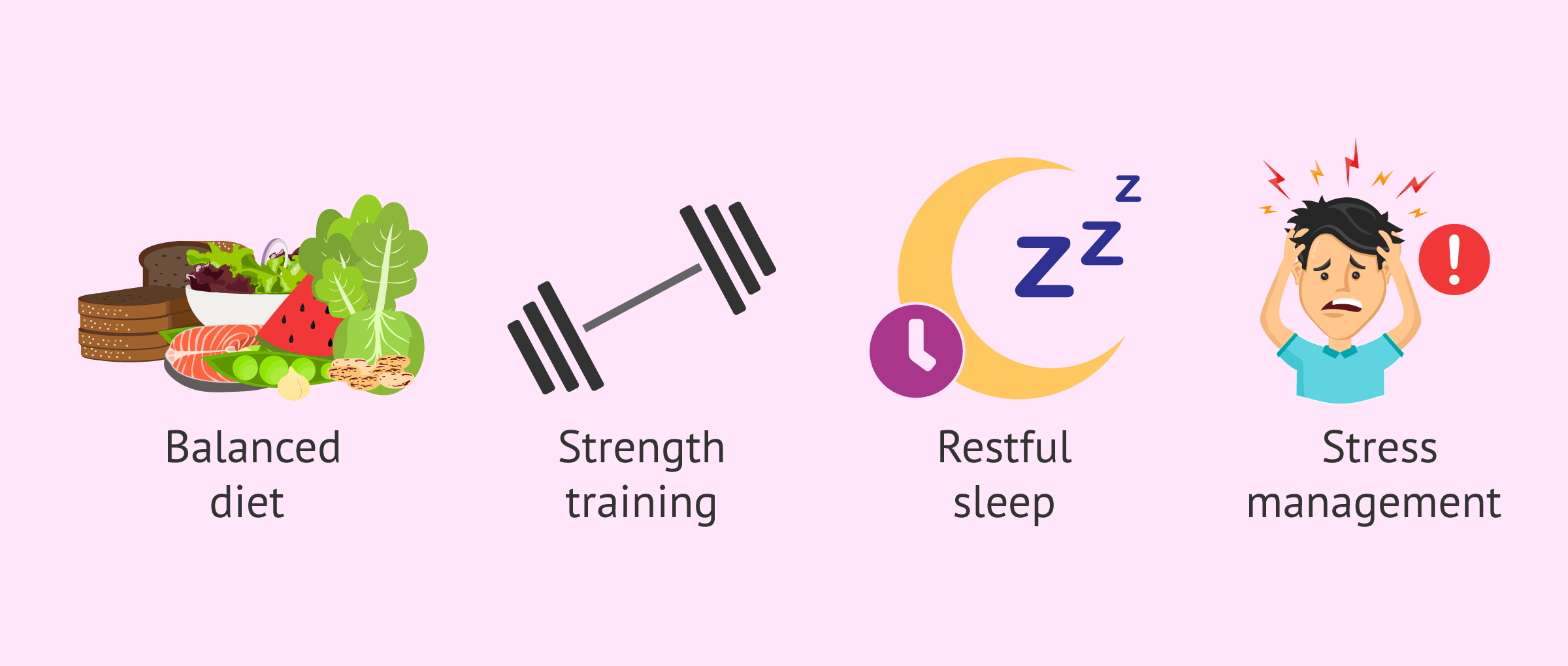
First, small lifestyle changes can optimize hormone production and increase testosterone levels. Some recommendations for this would be the following:
- Balanced diet: the consumption of healthy fats (omega-3, avocado, nuts) is essential, since testosterone is synthesized from cholesterol. Zinc and vitamin D are also key allies.
- Strength training: weightlifting and high-intensity interval training (HIIT) have been shown to naturally raise levels.
- Restful sleep: most testosterone is released during the REM phase of sleep. Sleeping less than 6 hours can drastically reduce its levels.
- Stress management: cortisol (the stress hormone) is the direct enemy of testosterone; when one goes up, the other goes down.
Ultimately, adopting these healthy habits is an excellent strategy to create a favorable environment that allows the body to regulate its own hormones. However, it is important to maintain realistic expectations.
Although lifestyle has a huge impact, it is not a miracle cure. If there is a severe clinical hormonal deficit (hypogonadism) or an underlying problem directly affecting fertility, sports and diet will not be enough on their own.
Testosterone drugs
There are several types of medications to give testosterone exogenously:
- Via gel
- Androgel, Testogel...
- Via patches
- Androderm, Testopatch...
- Via injections
- Reandron, Testex Prolongatum...
- Via implant or chip
- Rejuvchip

The doctor responsible for the treatment will choose the method of administration of testosterone according to the specific deficit and the characteristics of the man or woman.
Artificially administered testosterone can have side effects, so medical follow-up and dose control are very important. The most common adverse effects are breast enlargement, fluid retention, and prostate growth.
The latter is the most important risk, so doctors usually perform a specific prostate analysis before treatment to ensure that there is no tumor in the area, decreasing the likelihood of cancer occurring after abnormal prostate growth.
FAQs from users
What is the function of testosterone in men?
Mainly, testosterone plays two roles in the male body:
- Androgenic effect: contributes to the development and maintenance of male sexual characteristics (appearance of a beard, voice deepening, etc.)
- Anabolic effect: promotes an increase in bone mass and strength in men. Furthermore, this anabolic effect of testosterone in men causes the stimulation of bone growth and maturation.

What treatment options do I have for abnormal testosterone levels?
Artificial testosterone can be administered through different routes:
- Intramuscular injection: there exist different types of synthetic testosterone that can be administered intramuscularly. Propionate remains for a reduced time period in the body, so it has to be administered every 2-3 days. Testosterone enanthate and cypionate can be injected every two weeks (dose of 200 mg). Conversely, testosterone undecanoate can be administered every 12-15 weeks (1000 mg).
- Transfermal (patch): it can be administered in the form of a gel or cream daily, in the form of patches or implant.
- Oral (pills): this is the least common of all routes, since it is detrimental for the liver (hepatic toxicity).
Even though artificial testosterone can have many benefits, like muscle development or secondary male characteristics, one should keep in mind that, as with any other medication, it can have some side effects. Always follow your doctor's instructions before taking this type of medication.
What is the difference between total, free, and bioavailable testosterone?
When you receive a laboratory result regarding a hormonal analysis, it is common to see different types of testosterone. Understanding the difference between the different types of testosterone is key to an accurate diagnosis:
- Total testosterone: is the total amount of the hormone in the blood. However, this number alone can be misleading, as it groups both the testosterone that your body can use and the one that is "blocked".
- Free testosterone: is the smallest fraction that refers to the testosterone circulating without binding to proteins. Although it represents only 1-2% of the total, it is the one that actually performs biological functions, as it can enter the cells of your muscles, brain, or reproductive system to exert its function immediately.
- Bioavailable testosterone: is the sum of free testosterone and that bound to albumin. It is the hormone that your body can use quickly and effectively, that is, it is the total fraction of hormone that is actually "available" for your tissues to use in the short term.
Where is testosterone produced in women?
Although it is true that testosterone levels are lower in women than in men, this hormone is very important and necessary in both sexes. A woman produces around 300 micrograms of testosterone a day.
The production of testosterone in women occurs in the ovaries and the adrenal glands (approximately 25% of the testosterone in each of the glands) and the remaining 50% is produced by the peripheral conversion of androstenedione to testosterone.
Therefore, in addition to testosterone, there are other important androgens in women:
- Dihydrotestosterone, with high androgenic activity.
- Androstenedione, produced in the ovaries and adrenal glands.
- Dehydroepiandrosterone and its sulfate.
The latter, androstenedione, dehydroepiandrosterone, and its sulfate, are precursors and can be converted to testosterone and dihydrotestosterone to exert their androgenic function.
Suggested for you
If you want to know more about childbirth and its natural development, don't miss the following article: Male and Female Sex Hormones - Definition & Functions.
You may also be interested in reference values for testosterone and other sexual hormones in order to evaluate fertility. Read more about here:
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Davis SR, Wahlin-Jacobsen S. Testosterone in women--the clinical significance. Lancet Diabetes Endocrinol. 2015 Dec;3(12):980-92 (View)
Nagels HE. Androgens (dehydroepiandrosterone or testosterone) for women undergoing assisted reproduction. Cochrane Database Syst Rev. 2015 Nov 26;(11):CD009749 (View)
Nieschlag E, Nieschlag S. ENDOCRINE HISTORY: The history of discovery, synthesis and development of testosterone for clinical use. Eur J Endocrinol. 2019 Jun 1;180(6):R201-R212 (View)
FAQs from users: 'What is the function of testosterone in men?', 'What treatment options do I have for abnormal testosterone levels?', 'What is the difference between total, free, and bioavailable testosterone?' and 'Where is testosterone produced in women?'.




