What is Adenomyosis? Risks, Symptoms and Treatment
Adenomyosis, also known as internal endometriosis, is a uterine condition in which tissue from the inner layer of the uterus (endometrium) is found in the muscular layer (myometrium).
The exact cause of adenomyosis is unknown, but it is related to estrogen. Most cases resolve when a woman reaches the end of her reproductive stage, that is, menopause.
This uterine alteration and the associated changes can affect a woman’s fertility. Therefore, the treatment for adenomyosis will depend on whether the woman is trying to conceive or not, although age and symptoms will also be taken into account.
The different sections of this article have been assembled into the following table of contents.
Contents
- 1.
- 2.
- 3.
- 3.1.
- 4.
- 5.
- 6.
- 7.
- 7.1.
- 8.
- 8.1.
- 8.2.
- 8.3.
- 8.4.
- 8.5.
- 8.6.
- 8.7.
- 8.8.
- 8.9.
- 9.
- 10.
What are the endometrium and myometrium?
To understand what adenomyosis is, it's important to know these two uterine layers.
The endometrium is the innermost layer of the uterus and lines the uterine cavity. This layer is highly vascularized (i.e., has many blood vessels) because it prepares each menstrual cycle for a possible embryo implantation and potential pregnancy.
If embryo implantation does not occur, the endometrium sheds and is expelled with menstruation.
On the other hand, the myometrium is the muscular layer of the uterus and is responsible for uterine contractions during childbirth.
What is internal uterine endometriosis?
Internal endometriosis or adenomyosis is the presence of endometrial tissue within the uterine myometrium. Two types of adenomyosis are distinguished:
- Focal or localized adenomyosis
- with adenomyomas (foci or accumulations of endometrium in the myometrium), also known as Cullen's adenomyosis.
- Diffuse adenomyosis
- small and numerous endometrial crypts in the inner myometrium, frequently distributed in the posterior uterine wall, which causes the uterus to increase in size. This is the most common form of adenomyosis.


This condition is more frequent in women aged 35 to 50 but can also occur in younger women.
Causes of adenomyosis
The causes of this uterine condition are not clearly known. One proposed theory supports an invasion of endometrial cells into the myometrium that could be triggered by incisions, for example, following uterine surgery. Another theory suggests that adenomyosis is due to alterations during fetal development of the female reproductive system.
The most current theories explaining the origin of adenomyosis are based on the invasion of the myometrium by bone marrow stem cells.
Risk factors
Regardless of the origin of adenomyosis, what is clear is that this uterine condition is estrogen-dependent. Some of the factors that may predispose a woman to develop adenomyosis include:
- Previous uterine surgeries (C-sections, curettage, etc.)
- Multiple births.
- Women of reproductive age, especially those between 35–50 years old.

There may also be a genetic predisposition to adenomyosis.
Symptoms
A woman with adenomyosis may have no symptoms or only mild ones. However, about two-thirds of women with adenomyosis present some type of symptom. If symptoms occur, these are the most frequent clinical manifestations:
- Severe menstrual pain (dysmenorrhea).
- Prolonged or heavy menstrual bleeding (menorrhagia).
- Anemia caused by heavy bleeding.
- Pain during sexual intercourse (dyspareunia).
- Bleeding unrelated to menstruation (metrorrhagia).
- Lower back pain.
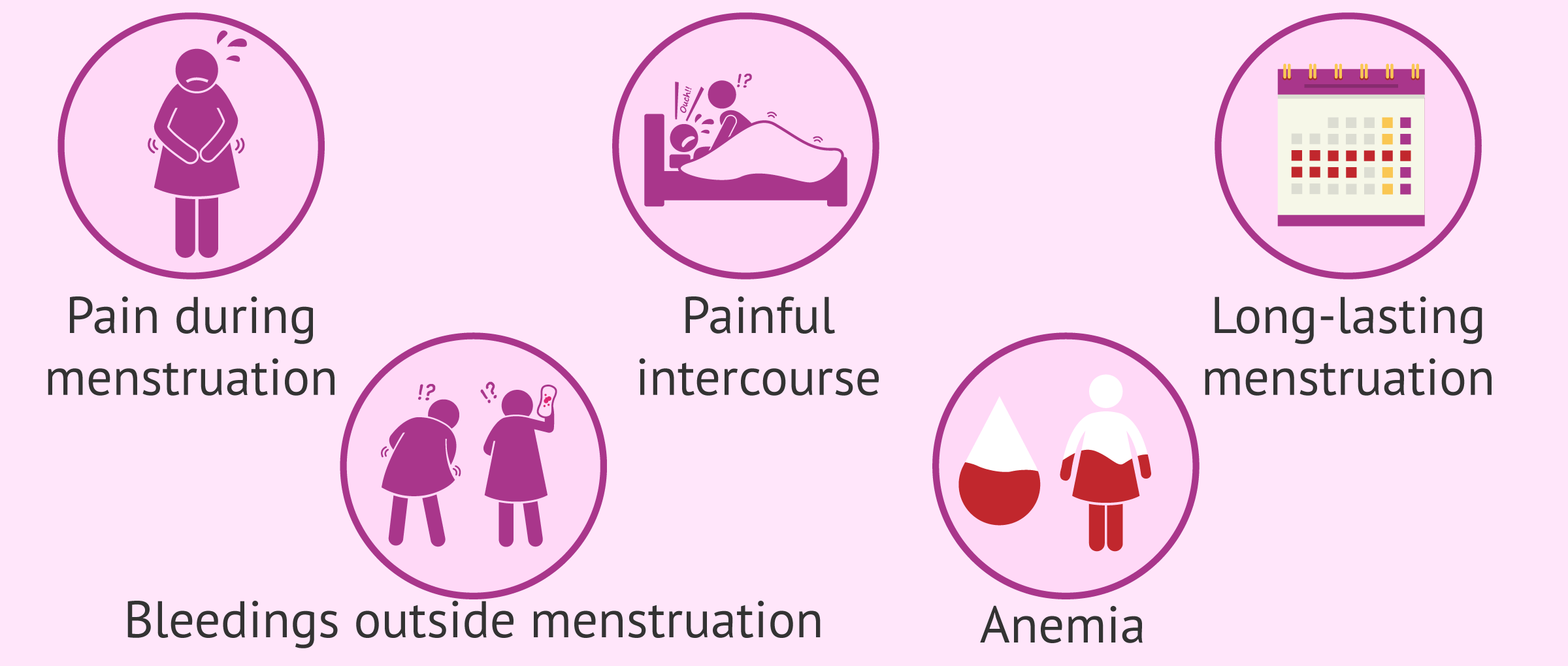
These symptoms affect the patient’s quality of life. However, symptoms associated with adenomyosis generally resolve after menopause.
How is adenomyosis diagnosed?
The clinical detection of adenomyosis is challenging because its symptoms are nonspecific and may also be caused by other uterine conditions. As a result, adenomyosis has been underdiagnosed until recently.
Thanks to technical improvements in ultrasound devices and increased awareness among specialists, adenomyosis is now diagnosed more frequently and accurately.
For diagnosis, it is important to rule out that the patient's symptoms are caused by another uterine condition. To reach a diagnosis of adenomyosis, specialists consider the patient’s medical history and may use various tests:
- Gynecological examination: may reveal an enlarged uterus.
- Transvaginal ultrasound: a simple and painless test that provides useful information for detecting adenomyosis.
- Magnetic resonance imaging (MRI): useful for complementing ultrasound findings to confirm diagnosis.
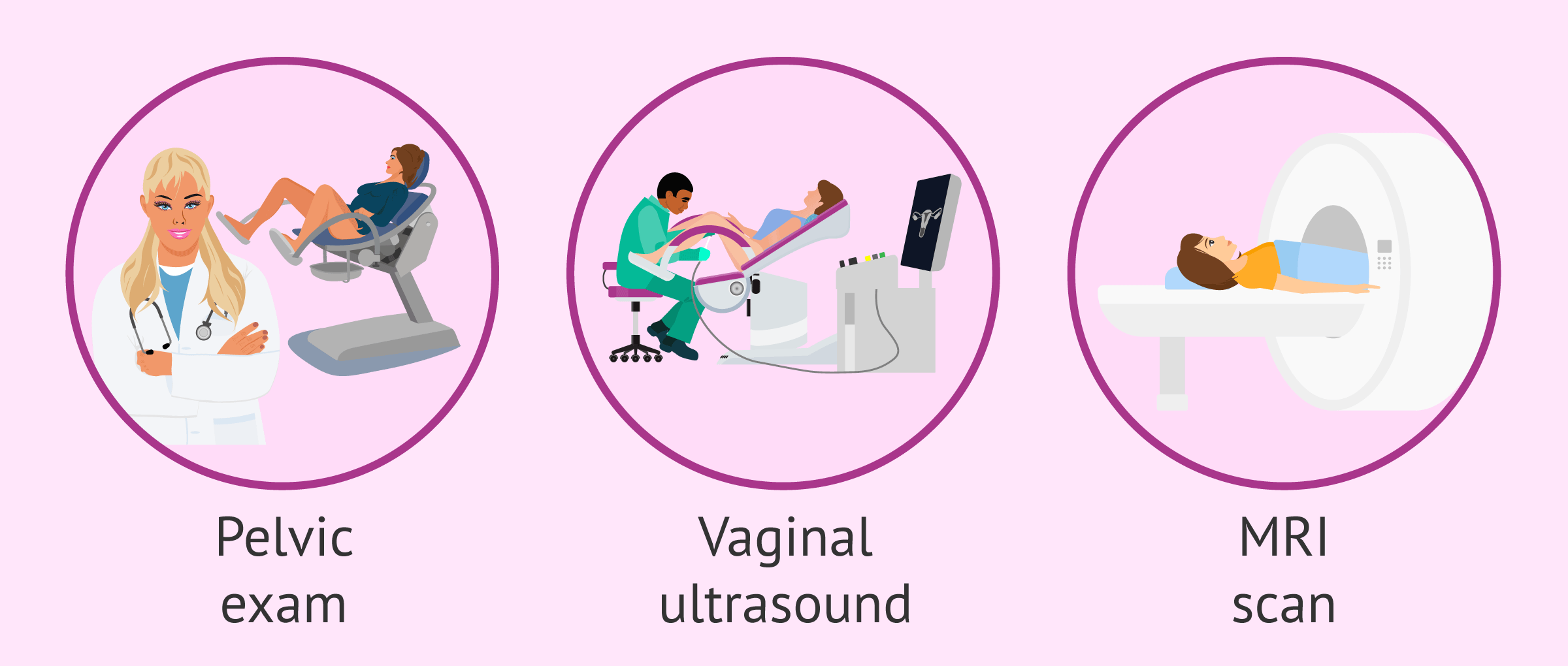
Other potentially useful tests for diagnosing adenomyosis include hysteroscopy, hysterosalpingography, and endometrial biopsy.
Nevertheless, the only technique that provides a definitive diagnosis of adenomyosis is histopathological examination of the uterus after a hysterectomy (partial or total removal of the uterus), although this is uncommon, especially in young women with fertility desires.
Is there a treatment for adenomyosis?
Treatment for adenomyosis should be individualized and will depend mainly on the severity of symptoms (mild, moderate, severe), fertility desires, and the patient’s age.
Treatment options include different medications:
- Anti-inflammatory drugs.
- Oral hormonal contraceptives.
- Intrauterine device (IUD).
- Gonadotropin-releasing hormone (GnRH) agonists.
Surgical treatment is also an option for adenomyosis. This may be conservative (removing or reducing endometrial tissue in the myometrium while preserving the uterus) or radical (removing the uterus).
Radical treatment is considered when symptoms are severe, medications are ineffective, and the woman is not close to menopause and does not wish to become pregnant.

Effects on fertility
Adenomyosis can have a negative impact on female fertility and cause problems in achieving pregnancy. A high percentage (up to 22–24%) of women with difficulty getting pregnant have adenomyosis.
Proposed mechanisms by which adenomyosis affects fertility include:
- The path of the sperm toward the egg may be hindered by structural changes and increased uterine size, as well as by abnormal contraction patterns. Even if fertilization occurs, embryo transport to the uterus for implantation may be impaired.
- Endometrial receptivity and embryo implantation may be affected, associating adenomyosis with implantation failure.

Thus, adenomyosis has been associated with:
- Ectopic pregnancy.
- Implantation failure.
- Spontaneous and recurrent miscarriage.
It is also important to mention that adenomyosis may occur alongside other conditions such as endometriosis or fibroids.
For all these reasons, an accurate diagnosis and a proper, individualized treatment can help a woman achieve pregnancy. This may involve the use of assisted reproductive technologies.
Adenomyosis and pregnancy
If a woman with adenomyosis wishes to conceive and has fertility problems, depending on her specific case, medical treatment, conservative surgical treatment, or both may be indicated. Personalization is essential, depending on each patient’s situation and type of adenomyosis...
In vitro fertilization (IVF) with a personalized protocol is an assisted reproduction technique that can also help when natural conception does not occur in women with adenomyosis. However, adenomyosis may affect IVF outcomes, with lower pregnancy and live birth rates and a higher miscarriage rate.
Additionally, once pregnancy is achieved, adenomyosis may affect the gestation and increase the risk of complications such as:
- Spontaneous miscarriage.
- Intrauterine growth restriction.
- Placenta previa.
- Preeclampsia.
- Preterm birth.
- Cesarean delivery.
- Postpartum hemorrhage.
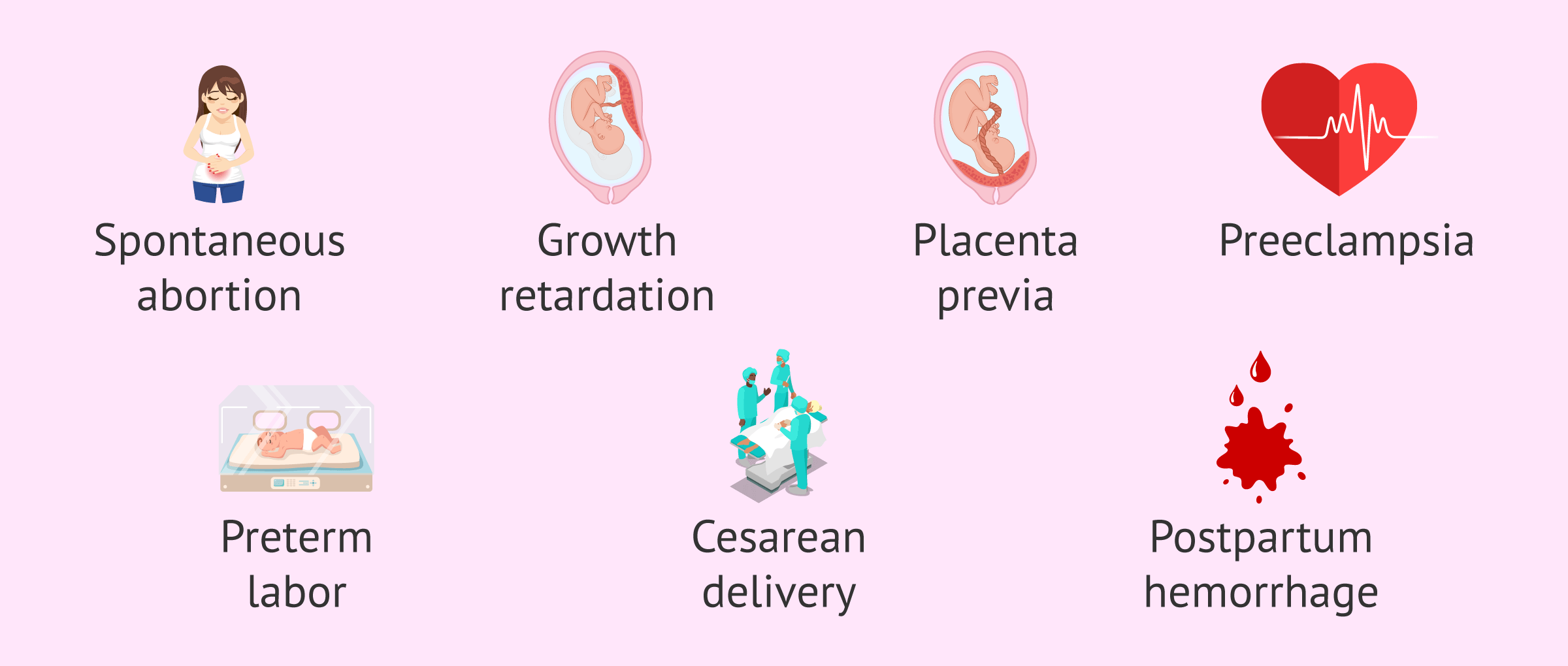
All of this makes it extremely important to have close pregnancy monitoring in cases of adenomyosis, to help prevent or detect these complications early.
FAQs from users
Is there a cure for adenomyosis?
Uterine adenomyosis is defined as an inadequate invasion of the tissue that normally lines the interior of the uterus, which has the function of allowing the implantation of the embryo and supporting the pregnancy for its entire duration, to the deepest layers of the uterus. This invasion can generate very painful periods, very heavy bleeding and in the case of fertility these invasive areas cause less blood to reach the endometrium (a phenomenon we call vascular sequestration) leaving the embryo with less available nutrients.
Outside the context of fertility it could be said that adenomatosis and its symptoms have a cure and it would be the removal of the uterus, but in our context this option is unthinkable, so all the solutions for us are to reduce the activity of this disease in order to improve the chances of pregnancy. These solutions go along two lines.

The first uses medications that reduce the activity of the adenomyosis before pregnancy. This has to be done in conjunction with assisted reproduction treatment since these medications inhibit ovulation. The second involves minimally invasive surgery such as radiofrequency ablation of the areas of adenomyosis. It is a very innovative treatment that is giving very good results.
Can obesity influence adenomyosis?
Adenomyosis, also known as internal endometriosis, is a uterine condition in which there is tissue from the inner layer of the uterus (endometrium) in the muscular layer of the uterus (myometrium). The causes of this condition are not clearly known, although it is known to be estrogen-dependent and, among the factors that predispose it to develop, we find having had at least one pregnancy and previous uterine surgeries (cesarean sections, curettage, hysteroscopies, etc.).
It is also very much related to age, especially after 40 years of age. That is why in some cases it is colloquially called uterine aging.
Certain adenomioses are only detected by special techniques such as a 4D ultrasound or a magnetic resonance imaging. For mild cases, there are very few treatments with apparent effectiveness and it is not fully demonstrated that they have a negative effect on patients' pregnancy rates. However, severe cases such as T-uteruses require corrective surgery through hysteroscopy.
Does adenomyosis produce cancer?
No evidence has been found that adenomyosis causes cancer. However, some symptoms of adenomyosis may be linked to some cancers, such as uterine bleeding.
Can women who haven't had children have adenomyosis?
This disorder is more common in women aged 40-50 who have already given birth, but it can also occur in younger women who have not yet become mothers.
Can I become egg donor if I have adenomyosis?
Each case has to be assessed individually. It must be taken into account that some of the symptomatic treatments for adenomyosis are hormonal and can complicate obtaining the eggs.
You'll find more information about the egg donation process here: How can I become an egg donor?
Is adenomyosis inherited?
No. Adenomyosis is not inherited. The exact possible cause of this condition is not known, but it is known that any woman of reproductive age and menstruation can develop adenomyosis.
Is uterine myoma (fibroids) the same as adenomyosis?
No. In the case of uterine myomatosis, fibroids, that is, tumors of muscle tissue, form. Adenomyosis, on the other hand, is the presence of endometrial tissue in the myometrium. They only coincide in location: the myometrium, the muscular layer of the uterus.
Is endometriosis the same as adenomyosis?
Both pathologies consist of the presence of ectopic endometrial tissue, that is, outside its physiological location: the endometrium.
However, a distinction must be made between internal endometriosis or adenomyosis and external endometriosis. In the former, the endometrial tissue is found in the myometrium. In the second, it can appear in any organ of the body other than the uterus.
Generally, when we refer only to endometriosis, we are talking about external endometriosis.
On the other hand, it is also important to note that, although they are not exactly the same pathology, some women can present both at the same time.
At what age is adenomyosis most common?
Adenomyosis is a condition that can appear in women at any age within the reproductive stage. However, this pathology is not usually frequent in women who have reached menopause.
In addition, adenomyosis is more common among women who have already been pregnant and have given birth.
Suggested for you
Adenomyosis is classified as a uterine disorder that may affect fertility. In this article you will find more information about this type of pathology and its influence on sterility: Uterine Factor female infertility.
If you want to know more about fibroids, we recommend you follow this link: What are fibroids?
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
References
Cunningham R, Horrow M, Smith R, Springer J. Adenomyosis: A Sonographic Diagnosis. Radiographics. Sep-Oct 2018;38(5):1576-1589. doi: 10.1148/rg.2018180080 (View)
Harada T, Khine YM, Kaponis A, Nikellis T, Decavalas G, Taniguchi F. The Impact of Adenomyosis on Women's Fertility. Obstet Gynecol Surv. 2016 Sep;71(9):557-68. doi: 10.1097/OGX.0000000000000346 (View)
Lacheta J. Uterine adenomyosis: pathogenesis, diagnostics, symptomatology and treatment. Ceska Gynekol. Spring 2019;84(3):240-246.
Osada H. Uterine adenomyosis and adenomyoma: the surgical approach. Fertil Steril. 2018 Mar;109(3):406-417. doi: 10.1016/j.fertnstert.2018.01.032 (View)
Pontis A, D'Alterio MN, Pirarba S, Angelis C, Tinelli R, Angioni S. Adenomyosis: a systematic review of medical treatment. Gynecol Endocrinol. 2016 Sep;32(9):696-700. doi: 10.1080/09513590.2016.1197200 (View)
Santulli P, Vannuccini S, Bourdon M, Chapron C, Petraglia F. Adenomyosis: the missed disease. Reprod Biomed Online. 2025 Apr;50(4):104837. doi: 10.1016/j.rbmo.2025.104837. PMID: 40287215. (View)
Somigliana E, Vigano' P, Invernici D, Fornelli G, Merli CEM, Vercellini P. Risk of endometriosis progression in infertile women trying to conceive naturally or using IVF. Hum Reprod. 2025 May 9:deaf090. doi: 10.1093/humrep/deaf090. Epub ahead of print. PMID: 40344687. (View)
Struble J, Reid S, A Bedaiwy M. Adenomyosis: A Clinical Review of a Challenging Gynecologic Condition. J Minim Invasive Gynecol. 2016 Feb 1;23(2):164-85. doi: 10.1016/j.jmig.2015.09.018 (View)
Vannuccini S, Petraglia F. Recent advances in understanding and managing adenomyosis. F1000Res. 2019 Mar 13;8:F1000 Faculty Rev-283. doi: 10.12688/f1000research.17242.1 (View)