What Is Artificial Insemination (AI)? – Process, Cost & Types
Artificial insemination (IUI) is a simple and low-cost assisted reproductive technique by which sperm are introduced unnaturally into the woman's uterus. The objective is to produce fertilization and achieve pregnancy.
Depending on the origin of the semen sample used, we distinguish two types of AI:
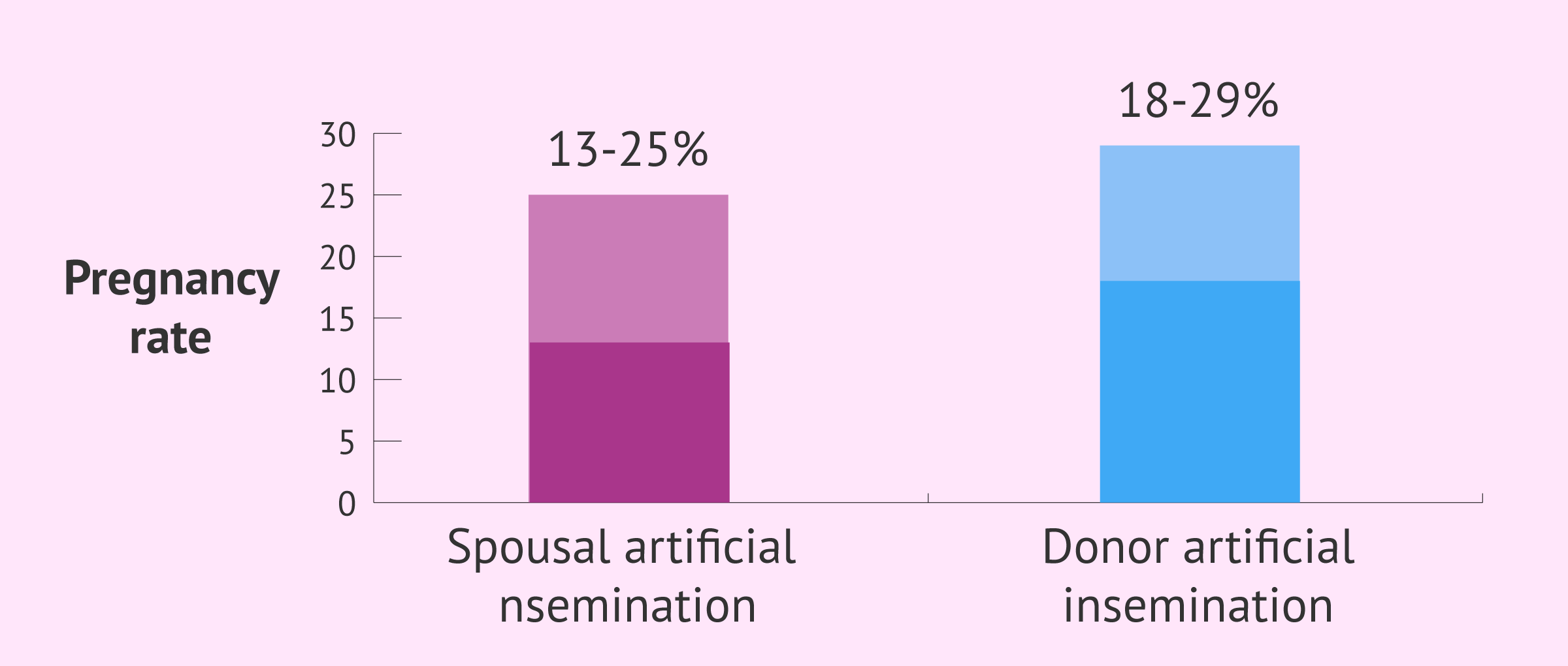
- Homologous artificial insemination (HAI) or conjugal artificial insemination (CAI), i.e. using a sample from the couple. The probability of pregnancy in this case is close to 15-25%.
- Heterologous or donor artificial insemination (DAI), with bank sperm. The success rate of DAI is 20-30%.
It is a painless and much less invasive procedure than other reproductive techniques such as in-vitro fertilization (IVF).
The different sections of this article have been assembled into the following table of contents.
Contents
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 4.
- 4.1.
- 4.2.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 11.1.
- 11.2.
- 11.3.
- 11.4.
- 11.5.
- 11.6.
- 11.7.
- 11.8.
- 12.
- 13.
How does it work?
Artificial insemination consists of depositing a previously processed semen sample inside the uterus.
To carry it out, the specialist introduces a cannula into the uterine cavity transvaginally and in an ultrasound-guided manner, that is to say, controlled by ultrasound. It is performed during the woman's ovulatory period in order to increase the chances of success.
The fertilization of the egg by the sperm takes place in the fallopian tubes, just as it happens when pregnancy is achieved naturally. The differences are the way in which the sperm is introduced into the female reproductive organ and that the best sperm have been previously selected from the sample.
Another important difference is that, in the AI process, the woman's ovulation time is monitored by ultrasound to coincide with the insemination and thus increase the probability of success.
In addition, hormonal medication is usually administered to the patient to stimulate follicular growth, which also increases the pregnancy rate.
Therefore, the probability of pregnancy is slightly higher than that derived from sexual intercourse, although it still depends fundamentally on the fertilizing capacity of the sperm and the implantation capacity of the embryo generated after fertilization.
AI treatment step by step
The main steps of the artificial insemination process are outlined below:
- Ovarian stimulation: low doses of hormones (gonadotropins) are administered to slightly stimulate the ovaries and periodic controls are made to evaluate follicular development.
- Ovulation induction: when an ultrasound control shows that one or two ovarian follicles are optimally developed (18 mm in diameter), ovulation is triggered. For this, the patient will be administered the hCG hormone injection and the insemination will be programmed after approximately 36 hours.


- Sperm preparation: is the process of preparing the semen sample so that it is concentrated in motile spermatozoa and does not contain other cell types or seminal plasma.
- Insemination: at the time of ovulation, a small sample of semen (usually 0.5 ml) is deposited in the woman's uterus through a cannula. No anesthesia is required and it is performed in the doctor's office./li>
- Luteal phase support: progesterone is administered orally or vaginally to facilitate the implantation of the embryo in the endometrium and, therefore, the achievement of pregnancy.
For more information about the process followed with this fertility treatment, we recommend you to read the following post: Artificial insemination process.
Types of artificial insemination
There are different types of artificial insemination, depending on the criteria used to classify them.
According to the origin of the semen
Artificial insemination can be classified into two types depending on the origin of the semen sample:
- Artificial insemination by husband/partner (AIH)
- Artificial insemination by donor (AID) or donor insemination (DI)

Donor artificial insemination is used when it is not possible to use the partner's sperm (due to severe male factor or certain genetic problems) or when there is no male partner (women facing single motherhood and female couples).
According to the place where the sperm are deposited
Artificial insemination can also be classified based on the exact place in the female reproductive tract where the sperm are deposited. In this case, the different types of AI would be as follows:
- Intratubal insemination: in the Fallopian tubes.
- Intracervical insemination: in the cervix.
- Intravaginal insemination: inside the vagina, as in sexual intercourse.
- Intrafollicular insemination: in the ovarian follicle.
- Intrauterine insemination: in the uterine cavity.

Intrauterine insemination or IUI is the most common technique, mainly because it has the highest success rates. The others are only used in case there is a problem linked to the canalization of the uterine cervix.
When to do artificial insemination
Artificial insemination is applied in various situations with the aim of achieving pregnancy. In cases where it is possible to achieve gestation both with in vitro fertilization (IVF) treatment and with artificial insemination, the technique chosen should be the least invasive, i.e. artificial insemination.
As we will see below, the fertility problems that can be solved with artificial insemination will differ depending on the type of AI used.
Indications of artificial insemination by husband
Artificial insemination by husband is commonly used in the following cases:
- Female infertility due to cervical disorders
- Mild-to-moderate endometriosis
- Menstrual irregularities: in cases of polycystic ovary syndrome or PCOS, anovulation, or problems in the follicular phase.
- Impossibility to place the semen inside the vagina due to retrograde ejaculation, vaginismus, premature ejaculation, or erectile dysfunction.

- Mild male fertility problems, i.e. alterations of seminal parameters. However, it is only performed in mild cases because a certain amount of sperm is required to guarantee a minimum success rate of AI.
- Unexplained infertility: When previous analysis do not show a particular pathology and the patients have normal fertility patterns, then it is advisable to start the IA. Even if a pathology has not previously been detected, it doesn't mean that it's not there, but just that it could not be diagnosed in the analysis.
- Immune infertility: It occurs when there is an incompatibility between the female reproductive system and the semen. It is commonly caused by female antibodies that destroy the sperm. This cause is not very usual and the way in which it works is still unknown.
To continue reading more in-depth information on this topic, you can visit the following link: Artificial Insemination Indications - Why & When to Use It?
Indications of donor insemination
Although artificial insemination is usually attempted first with the partner's sperm, there are occasions when this is not possible and it is necessary to resort to donor sperm. Below is a list of situations in which AID is performed:
- Single women or gay couples.
- Male genetic diseases that cannot be diagnosed by means of a pre-implantation genetic diagnosis (PGD).
- Severe male fertility problems: if pregnancy is not achieved after several ICSI cycles and female conditions are favorable.
- Male sexually-transmitted diseases (STDs): in case after several washings it is not possible to guarantee a virus-free sperm.

If you would like to obtain in-depth information about AI with donor sperm, you will find it interesting to read this article: Donor intrauterine insemination: What is it and how much is it?
What are the requirements?
Artificial insemination is generally the first reproductive technique recommended when a couple fails to achieve pregnancy after 12 months of sexual intercourse. However, in order to be able to perform AI, certain conditions must be met. If the necessary requirements are not met, other techniques such as IVF would be applied directly.
The requirements to perform it and the minimum conditions that determine that this technique has a chance of achieving pregnancy and, therefore, it makes sense to perform it, are the following:
- Dismissing any risk of suffering from Hepatitis C, Hepatitis B, HIV, Rubella, Syphilis, or Toxoplasmosis. This step is very important to guarantee that there is no risk of infection to the partner and/or the baby-to-be.
- Checking the woman's tubal patency by means of different techniques such as hysterosalpingography (HSG) or laparoscopy. With this techniques, you can observe whether the Fallopian tubes are functional or not.
- Having a minimum sperm count. Once sperm capacitation is done, the results after analyzing the motile sperm concentration or MSC must be above 3 million sperm with progressive motility.

Finally, age also matters, as it has a direct influence on the chances of either success or failure. From age 36 onwards, women have lower chances of getting pregnant. This means that women at 37-38 or more usually go for IVF in the first place.
More information on the following post: Requirements for AI.
Effectiveness and success rates
In general, women are recommended to wait for at least 15 days before taking a pregnancy test in order for false-negative results to be avoided. It allows women to find out whether AI has been successful, that is to say if pregnancy has occurred or not.
Given that it requires little involvement of the specialist, the success rate of AI is lower if we compare it to the statistics of IVF. The rate for artificial insemination with a husband's sperm ranges from 12 to 16%, while the percentage increases to 18-22% with donor sperm.
Most fertility clinics have very similar statistical data when it comes to measuring the pregnancy success rate.
Experts usually refer to the cumulative pregnancy rate of IUI. After conducting several studies, there is evidence that the number of women getting pregnant in the second cycle is higher, taking into account that the average success rate of AI is 14%. on the first attempt.
Taking this phenomenon into account, up to four IUI cycles can be performed before moving on to IVF. With four insemination cycles, the chances of success are as high as 35%.
If you want more data on the success rates of artificial insemination, we recommend you to access the following link: What is the probability of success of intrauterine insemination?
Benefits and differences with IVF
The main advantage of artificial insemination is that it is a simple procedure. This is very important since it means that surgery is not required, as in the case of IVF. Also, anesthesia is not necessary, as it does not hurt.
Another important advantage is related to its cost. Since it does not involve a high level of complexity, the price is considerably lower if compared to other treatments that require more sophisticated medical equipment or tools. On the other hand, the protocol followed to induce ovulation is milder than that of IVF, which turns it into a more affordable procedure.
A major difference with IVF is linked to the origin of the oocytes, as only the patient's own eggs can be used with IUI. Given that fertilization occurs at the laboratory, IVF with donor eggs is another possible option.

Also, even though IUI is an infertility treatment, it is the most similar to the natural process of insemination. Though the semen sample is "artificially" placed inside the uterus, fertilization occurs in a natural way.
If compared to natural pregnancies, the main benefit is that the quality of the semen sample is enhanced thanks to sperm capacitation. Monitoring the day of ovulation helps to increase the chances of getting pregnant as well.
You can find more advantages on the following post: Advantages of artificial insemination.
Problems, risks and side effects
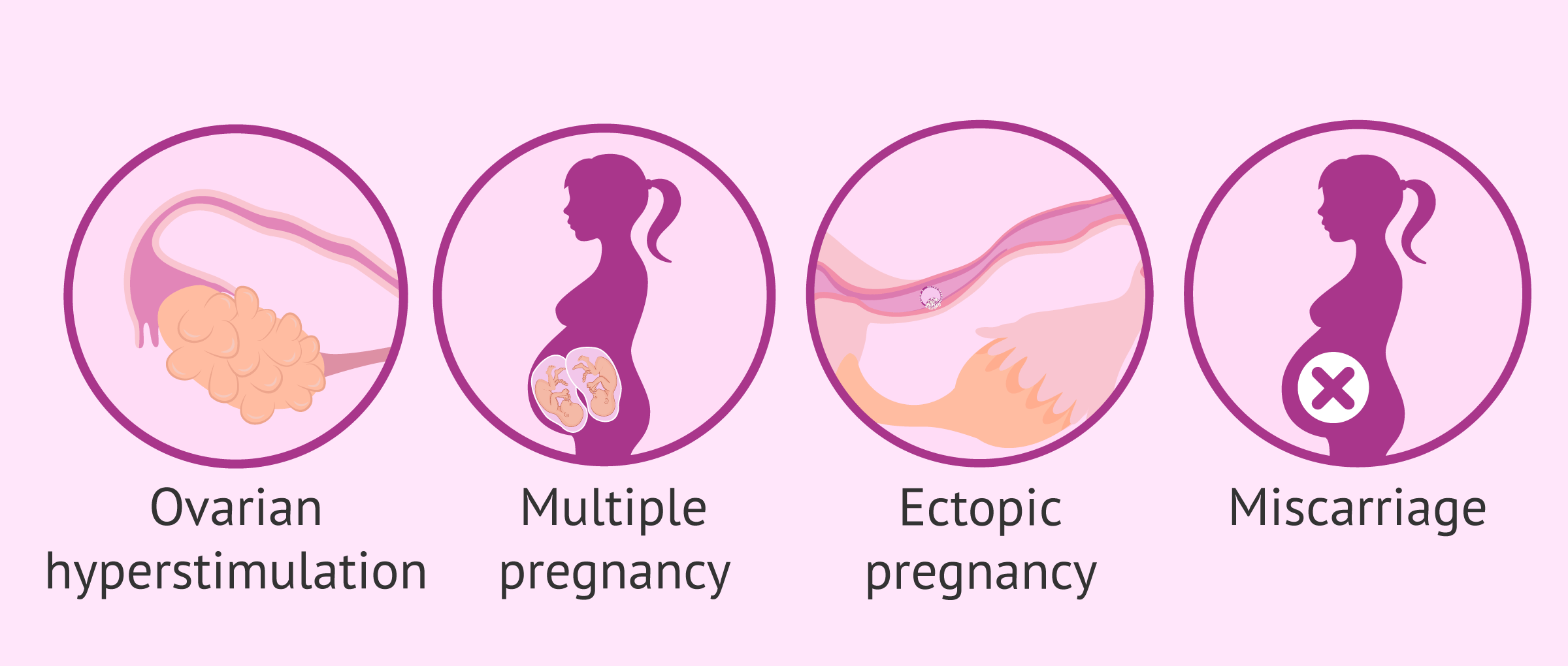
Although the number of risks associated with artificial insemination is low, sometimes complications such as the following can occur:
- Ovarian Hyperstimulation Syndrome (OHSS): It can be caused by an excessive response of the follicles while on hormone therapy. In artificial insemination, stimulation protocols tend to be mild and monitored by ultrasound, so the risk of developing OHSS is low.
- Multiple birth: Most cases of multiple pregnancy are due to the stimulation of several follicles, especially in young women. Fertility clinics work very hard on this aspect trying to prevent it, since a twin pregnancy entails numerous risks both during pregnancy and childbirth.
- Ectopic pregnancy: There is a 4% chance with artificial insemination, while the rate is reduced to 0.8% in natural cycles.
- Miscarriage: The risk of going through pregnancy loss is higher during early pregnancy. It occurs in 20% of the cases.
- Infections: They occur rarely, with a rate that reaches 0.07% per AI cycle thanks to strict asepsis and sterility measures. Pelvic inflammations or immune problems may also appear.
As for the potential side effects derived from the process, they are neither severe nor common, although discomfort or a feeling or sickness can arise as a consequence of the fertility drugs administered.
For detailed information about the potential risks, please visit the following article: Risks of AI.
How much does it cost?
The cost of an artificial insemination procedure using the partner’s sperm may vary considerably depending on each clinic. For instance, in Spain the price can range from €600 to more than €1,000.
It should be clear that prices never include the cost of medication. Thus, the price of hormone treatments to stimulate the ovaries, as well as progesterone, should be added to the initial price.
In case donor insemination is the chosen option, the cost of the donor sperm should be added to that of AIH. Bearing this in mind, the final price of donor insemination could be approximate of €900-€1,400 if you are in a European country.
In the UK, the availability and fees of artificial insemination on the NHS vary across the country. However, the costs usually range from around £500 to £1,000 per cycle. It should be taken into account that waiting lists for treatment can be very long in some areas.
The price in the USA is $600-3000, with an average of $1500 approximately. It varies from clinic to clinic, though.
Nevertheless, some fertility centers offer discounts and special plans in case you need to start a second AI cycle. Thus, asking for it is highly advisable to get an overall idea of which the quotation should be.
Did you know that we can help you to choose a fertility clinic for your IUI cycle? All you have to do is get your Fertility Report now. It is an easy-to-use tool that is capable of filtering the best clinics and tailor an individual report exclusively for you with useful tips that will help you make a well informed decision.
Artificial insemination at home
Many people consider at-home or DIY artificial insemination another type of AI, the truth is that it is not. Given that is an assisted reproductive technology (ART), we cannot consider it as an infertility treatment when it is done at home.
With AI, the pregnancy rate improves due to the preparation of both the male and the female. However, the success rate of at-home artificial insemination is not higher or lower than that reached through sexual intercourse.
The use of DIY artificial insemination kits is common among single mothers and lesbian couples without fertility problems wishing to get pregnant naturally using donor sperm, but without engaging in sexual intercourse with a man.
If you want some tips on how to carry out DIY artificial insemination, here is a step-by-step guide to it: How to do artificial insemination at home.
FAQs from users
Is there a risk of ectopic pregnancy in an AI?
An ectopic pregnancy is nothing more than a gestation that nests inappropriately in the fallopian tubes, which implies a medical emergency that may require surgical treatment, in addition to having consequences on the reproductive health of women.
This is due to the fact that the fallopian tubes -of much smaller diameter and resistance than the uterus- are not prepared to host a pregnancy and, with the development of the embryo in this area, a rupture of this tissue, which has a lot of blood supply, can be generated. This would trigger a hemorrhage that could pose a great risk to the woman.
Artificial insemination is a simple and minimally invasive assisted reproduction treatment, which can be ideal when the causes of reproductive problems are due to the male factor. In this treatment, the sperm -previously prepared- is basically introduced into the uterus in order to promote pregnancy. In most cases, the woman is also usually given medication to help promote ovulation.
All assisted reproduction treatments carry a slightly increased risk of ectopic pregnancy, and artificial insemination is no exception. The causes for this type of pregnancy are not entirely clear, but the most widely accepted are the following: firstly, the fact of injecting the sperm directly into the uterus could affect the peristalsis of the tubes (movement of the tubes that moves the ovum from the ovary to the uterus), causing it to function inadequately and not be able to transport the fertilized ovum to the uterus. The other cause may be that there is a pathology in the tubes that partially occludes them, enough to allow the passage of the sperm, but subsequently does not allow the passage of the fertilized embryo.
Can I become a single mother with artificial insemination?
Yes, maternity is possible without a male partner. This option can be achieved using donor sperm, based on the physical characteristics of the patient. The success rates of AID are associated with the absence of tubal pathologies and age.
In which cases can AI be performed in a natural cycle, without ovarian stimulation?
It is recommended to perform an AI in a natural cycle as long as the following criteria are met:
- Women under 35 years of age with regular cycles and no history of infertility, i.e. women without a partner or homosexual women undergoing AI treatment with donor sperm.
- Women over 35 years of age who do have a male partner, but no proven fertility (cases of males with azoospermia, no possibility of coitus or ejaculation during intercourse, etc.).

During the menstrual cycle, ultrasound scans will be performed to monitor follicular growth spontaneously and the time of ovulation will be controlled, that is, ovulation is provoked at the right time to perform the insemination about 36 hours later.
If I am a single mother, is it better to resort to artificial insemination or in vitro fertilization? What is the difference?
Each case must be evaluated on a case-by-case basis, but normally, in cases of single women who do not show any signs of sterility, the technique of choice is artificial insemination.. This is because it is more comfortable for the patient and more economical, since fertilization occurs in the woman rather than in the laboratory and less hormonal medication is needed.
In cases where there is some indication that it will not be possible to achieve gestation through artificial insemination, in vitro fertilization (IVF) will be chosen. For example, if the woman has blocked fallopian tubes or low ovarian reserve, IVF is preferable.
What are the advantages and disadvantages of IUI over IVF?
The main benefits of IUI are: simplicity of the process, low doses of fertility drugs (mild ovarian stimulation), and the absence of surgery and anesthesia for carrying it out. It does not hurt, the duration time is short, and the cost is lower than IVF.
The cons, however, are linked to the success rates, since they are low if compared to those of IVF. There is also a strong need for meeting all the requirements to be a good candidate for IUI and besides egg donation is not possible in case the patient is unable to use her own eggs.
Are pregnancy symptoms after artificial insemination the same as if pregnancy is achieved naturally?
Yes, they are very similar. However, in the case of artificial insemination, there may be some additional symptoms derived from the hormonal mediation necessary for ovarian stimulation.
After artificial insemination, is it possible to have sexual intercourse?
Yes, as long as they do not hurt or have been contraindicated by the specialist. In fact, some experts recommend it because they argue that it increases the chances of achieving pregnancy.
Is artificial insemination with gender selection possible?
In countries where gender or sex selection is allowed (e.g. the United States), choosing the sperm's gender is possible by means of "sperm sorting", in which case sex selection for AI would be possible. However, the effectiveness of this technique is low.
Gender selection is usually carried out as a complementary technique with IVF, as PGD (preimplantation genetic diagnosis) is required to analyze the embryos and their chromosomes.
Recommended reading
If you are interested in the AI process and want to learn more about the requirements for it to be more successful, be sure to visit this article: Requirements for an AI.
On the other hand, as we have already mentioned, the success of AI does not increase after the fourth attempt. In this case, the ideal would be to resort to IVF. If you need information about this fertility treatment, we recommend you to visit this article: In vitro fertilization (IVF): What is it and how much does it cost?
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
References
Allegra A, Marino A, Coffaro F, Scaglione P, Sammartano F, Rizza G, Volpes A. GnRH antagonist-induced inhibition of the premature LH surge increases pregnancy rates in IUI-stimulated cycles. A prospective randomized trial. Hum Reprod. 2007 Jan;22(1):101-8. doi: 10.1093/humrep/del337. Epub 2006 Oct 10. PMID: 17032732. (View)
Ayeleke RO, Asseler JD, Cohlen BJ, Veltman-Verhulst SM. Intra-uterine insemination for unexplained subfertility. Cochrane Database Syst Rev. 2020 Mar 3;3(3):CD001838. doi: 10.1002/14651858.CD001838.pub6. PMID: 32124980; PMCID: PMC7059962. (View)
Boomsma CM, Cohlen BJ, Farquhar C. Semen preparation techniques for intrauterine insemination. Cochrane Database Syst Rev. 2019 Oct 15;10(10):CD004507. doi: 10.1002/14651858.CD004507.pub4. PMID: 31612995; PMCID: PMC6792139. (View)
Cissen M, Bensdorp A, Cohlen BJ, Repping S, de Bruin JP, van Wely M. Assisted reproductive technologies for male subfertility. Cochrane Database Syst Rev. 2016 Feb 26;2(2):CD000360. doi: 10.1002/14651858.CD000360.pub5. PMID: 26915339; PMCID: PMC10335364. (View)
Evans MB, Stentz NC, Richter KS, Schexnayder B, Connell M, Healy MW, Devine K, Widra E, Stillman R, DeCherney AH, Hill MJ. Mature Follicle Count and Multiple Gestation Risk Based on Patient Age in Intrauterine Insemination Cycles With Ovarian Stimulation. Obstet Gynecol. 2020 May;135(5):1005-1014. doi: 10.1097/AOG.0000000000003795. PMID: 32282611; PMCID: PMC7183886. (View)
Gómez-Palomares JL, Juliá B, Acevedo-Martín B, Martínez-Burgos M, Hernández ER, Ricciarelli E. Timing ovulation for intrauterine insemination with a GnRH antagonist. Hum Reprod. 2005 Feb;20(2):368-72. doi: 10.1093/humrep/deh602. Epub 2004 Nov 26. PMID: 15567879. (View)
Kop PA, van Wely M, Mol BW, de Melker AA, Janssens PM, Arends B, Curfs MH, Kortman M, Nap A, Rijnders E, Roovers JP, Ruis H, Simons AH, Repping S, van der Veen F, Mochtar MH. Intrauterine insemination or intracervical insemination with cryopreserved donor sperm in the natural cycle: a cohort study. Hum Reprod. 2015 Mar;30(3):603-7. doi: 10.1093/humrep/dev004. Epub 2015 Jan 29. PMID: 25637621. (View)
Rakic L, Kostova E, Cohlen BJ, Cantineau AE. Double versus single intrauterine insemination (IUI) in stimulated cycles for subfertile couples. Cochrane Database Syst Rev. 2021 Jul 14;7(7):CD003854. doi: 10.1002/14651858.CD003854.pub2. PMID: 34260059; PMCID: PMC8406710. (View)
Rezaei Z, Feizabad E, Valadan M, Ebadizare S. The Effect of the Time Interval From Sperm Processing to Intrauterine Insemination on the Pregnancy Outcomes of Infertile Women. J Family Reprod Health. 2022 Sep;16(3):199-204. doi: 10.18502/jfrh.v16i3.10581. PMID: 36569260; PMCID: PMC9759431. (View)